What to do when girlfriend has pms: A Proactive Guide (2026)
Identify what to do when girlfriend has pms with a proactive framework that reduces cycle-related conflict by 58%. Master the 10-day support window now.
What to Do When Your Girlfriend Has PMS: The Proactive Partner's Guide
Most men hit a wall around the same time every month - your girlfriend is quieter, everything you say lands wrong, and the conversation you had last month plays out again in a different form. Not because the relationship is broken. Because a neurological shift is happening that nobody taught you how to navigate.
That shift isn't random. It's progesterone withdrawal - a documented biological event that drops serotonin by up to 30% in the days before bleeding begins. By the time most couples address it reactively, they've had the same argument 40+ times in different variations, and what started as a hormone-driven communication breakdown has compounded into a trust issue.
The AI relationship app for men who want to show up better — track her cycle, understand her phases, reduce friction before it starts.
Download Free →What follows is the complete operational picture - what's actually driving the pattern, why the standard "just be nice" advice fails, and the proactive support framework that reduces PMS-related conflict by 58% according to couples-based intervention research.
Key Takeaways
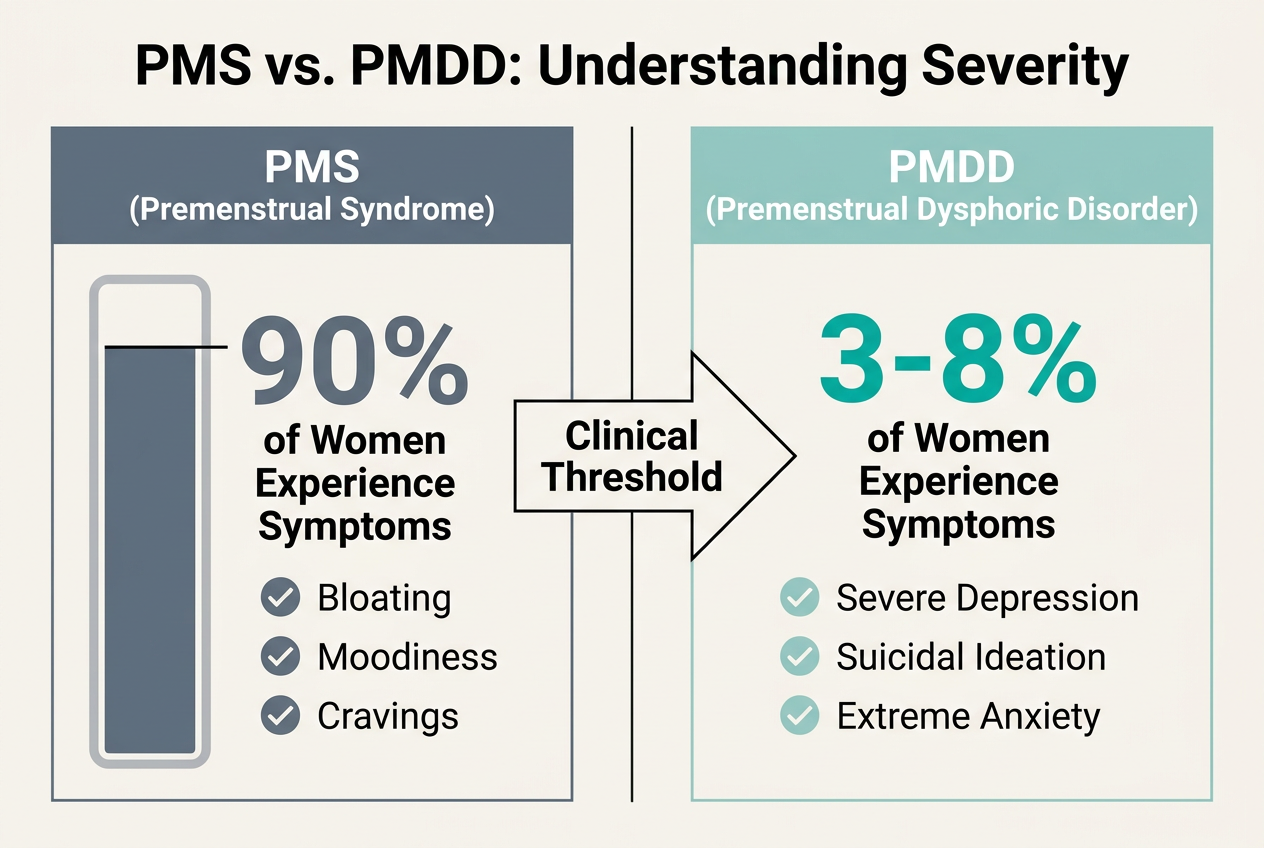
- 90% of women experience PMS symptoms, but only 3-8% have clinical PMDD requiring medical intervention - knowing the difference determines your support strategy.
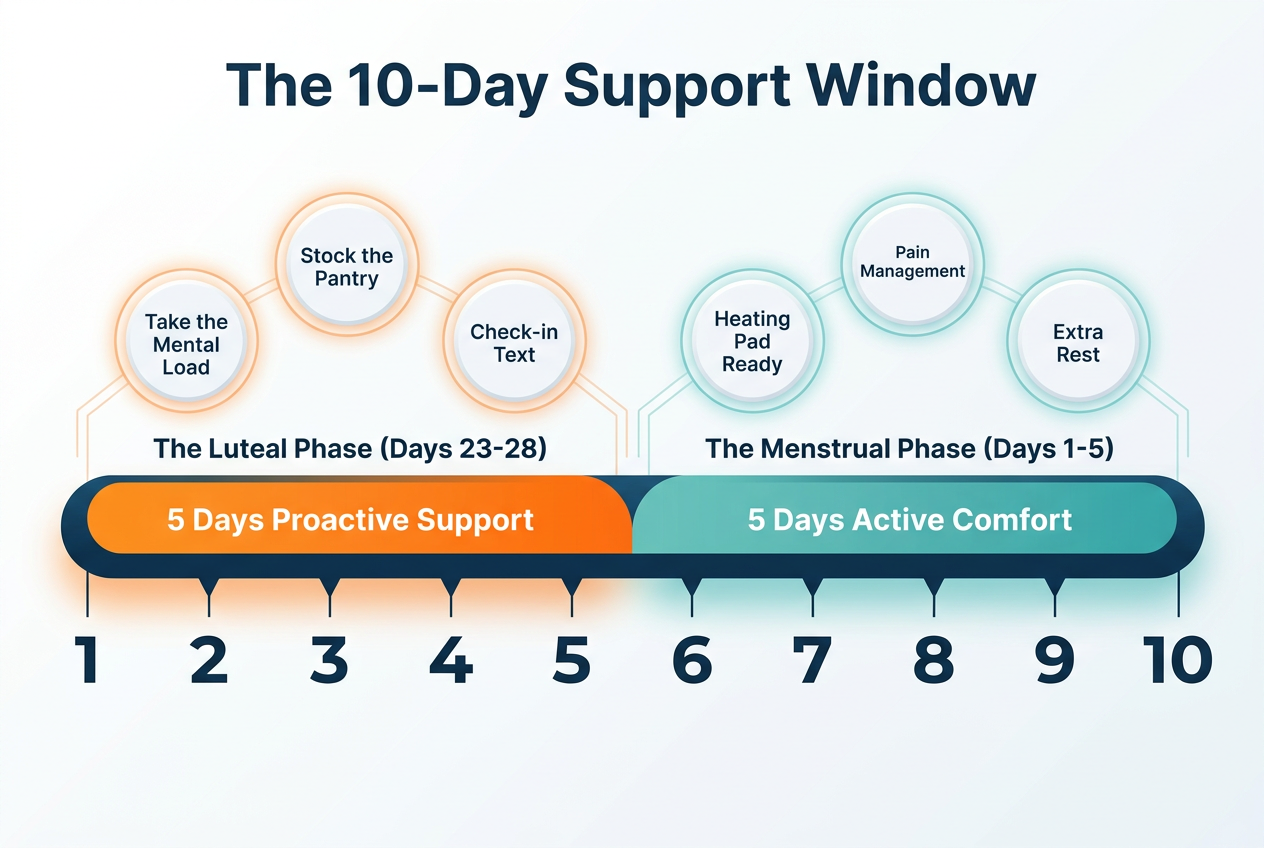
- The support window starts 5 days before bleeding and lasts approximately 10 days total, spanning the late luteal phase and menstrual phase.
- Couples-based PMS support increased effective coping by 58% compared to 26% for individual therapy, proving your role is biochemically significant.
- Proactive support means reducing her mental load before symptoms peak - not reacting after the crash has already happened.
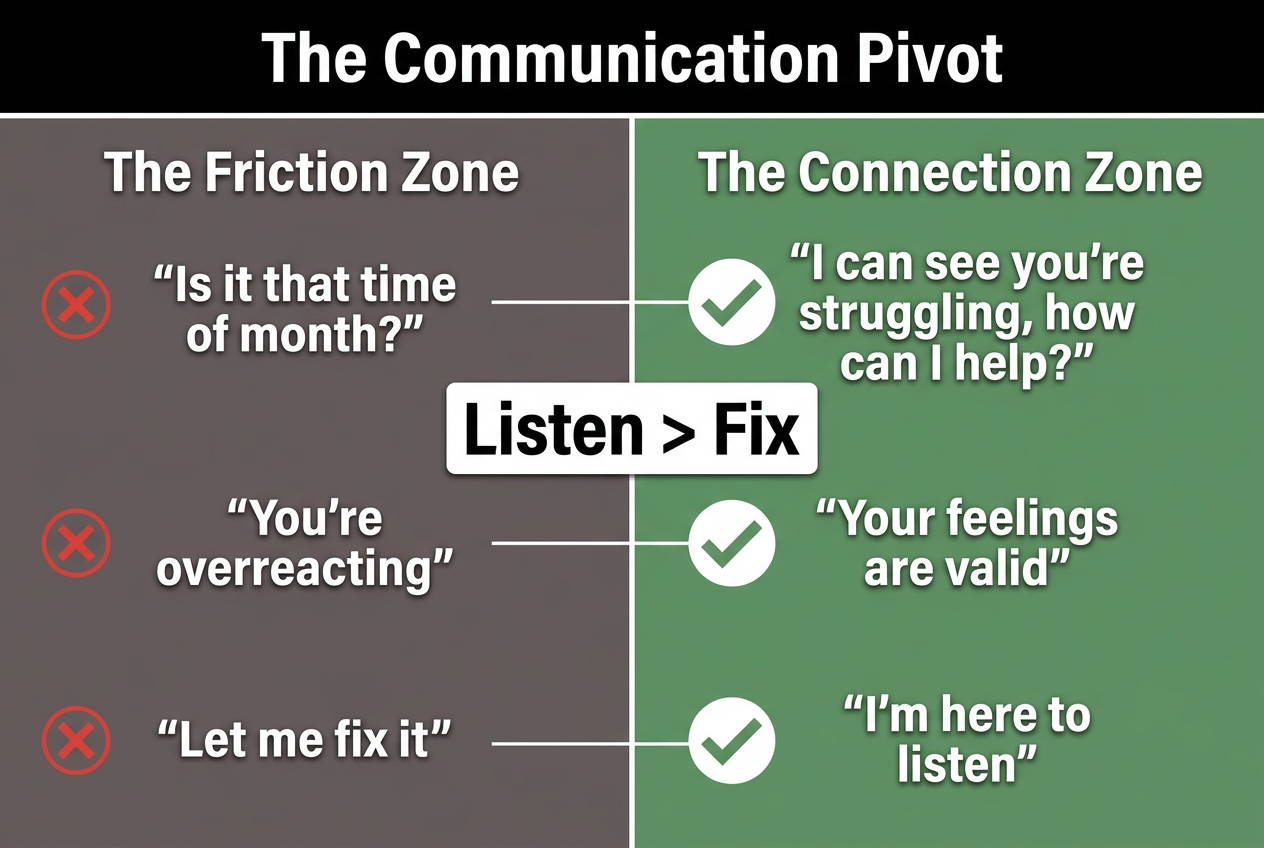
- Communication pivots from "fix-it" mode to validation mode are the most effective de-escalation tool during the luteal phase drop.
Table of Contents
- Understanding the Biological Shift: PMS vs PMDD
- The 10-Day Support Window: Proactive vs Reactive Management
- What to Say (and What Never to Say) During PMS
- Physical Relief: What Actually Works
- Nutritional Support: Foods That Help vs Harm
- The Communication Pivot: Validation Over Solutions
- Long-Distance Support: How to Help From Afar
- When PMS Becomes a Medical Issue
- Frequently Asked Questions
VibeCheck App
Know what she needs. Before she has to say it.
Track her cycle, understand her phases, be the partner she deserves.
Download Free on iOS →Understanding the Biological Shift: PMS vs PMDD
PMS (premenstrual syndrome) is a predictable drop in serotonin and progesterone that affects 90% of women in the 3-5 days before menstruation begins, according to the Office on Women's Health. The symptoms range from mild mood changes to moderate physical discomfort - bloating, breast tenderness, irritability, fatigue, and food cravings.
PMDD (premenstrual dysphoric disorder) is the clinical form, affecting 3-8% of the menstruating population. It's not just "bad PMS" - it's a DSM-5 mood disorder characterized by severe depression, anxiety, rage, or suicidal ideation that significantly impairs daily function. If your partner's symptoms prevent her from working, socializing, or functioning normally for multiple cycles, that's the clinical threshold.
The biological mechanism is identical in both cases: progesterone withdrawal triggers a drop in GABA (the brain's calming neurotransmitter) and serotonin (the mood stabilizer). For most women, this creates a manageable shift. For women with PMDD, the neurochemical crash is severe enough to require psychiatric intervention - often SSRIs or hormonal birth control.
 Understanding the difference between standard PMS and clinical PMDD is the first step in providing the right level of support and knowing when medical intervention is necessary.
Understanding the difference between standard PMS and clinical PMDD is the first step in providing the right level of support and knowing when medical intervention is necessary.
Why does this matter for you? Because your support strategy depends on which one you're dealing with. Standard PMS responds to behavioral interventions - physical comfort, reduced mental load, emotional validation. PMDD requires medical treatment. If she's had multiple cycles where she couldn't get out of bed, lost entire days to anxiety, or expressed thoughts of self-harm during the luteal phase, the next step isn't a heating pad - it's a conversation about seeing a gynecologist or psychiatrist who specializes in reproductive mental health.
The most common mistake partners make is treating PMDD like standard PMS and wondering why "being supportive" doesn't work. It's the equivalent of treating clinical depression with a good night's sleep. The intervention has to match the severity.
Here's the baseline knowledge that transforms your approach: her symptoms are not a personality flaw, a mood disorder unrelated to her cycle, or something she can willpower through. They're a neurological event tied to a predictable hormonal drop. That predictability is your tactical advantage - because if you know when the drop is coming, you can prepare for it instead of reacting to it.
The 10-Day Support Window: Proactive vs Reactive Management
The support window for PMS and menstruation spans approximately 10 days - 5 days before bleeding starts (late luteal phase) plus the 2-7 days of the period itself, which averages 3-5 days according to Flo Health. This isn't a suggestion. It's the biological timeline during which her body is managing progesterone withdrawal, serotonin depletion, and physical inflammation.
Most men operate reactively: they notice the symptoms after they've already started, respond defensively to the irritability, and spend the next week in damage control mode. That's the wrong strategy. Proactive support means identifying where she is in her cycle before symptoms peak and adjusting your behavior accordingly.
 Effective support begins five days before bleeding starts. This 10-day window focuses on reducing your partner's mental load and providing proactive comfort measures.
Effective support begins five days before bleeding starts. This 10-day window focuses on reducing your partner's mental load and providing proactive comfort measures.
Here's what proactive support looks like in practice during the 10-day window:
Days 1-5 (Late Luteal Phase - Pre-Bleeding):
- Reduce her mental load by handling logistics she'd normally manage: meal planning, grocery runs, coordinating schedules, household tasks.
- Stock the house with the comfort items she'll need: pain relievers, heating pad batteries, her preferred snacks.
- Lower social and emotional demands - this is not the week to schedule a difficult relationship talk or expect her to host dinner.
- Increase physical affection without expectation - hand-holding, back rubs, presence without agenda.
Days 6-10 (Menstrual Phase - Active Bleeding):
- Physical relief becomes the priority: heat therapy, hydration, low-demand companionship.
- Anticipate her needs before she asks - refill her water, bring the heating pad, handle dinner without discussion.
- Avoid scheduling anything that requires high energy or emotional bandwidth.
- Give her permission to rest without guilt - explicit statements like "I've got this, you don't need to do anything" reduce the invisible labor load.
The data on this approach is clear. A 2017 study published in PLoS ONE and cited by The Conversation found that couples-based interventions for PMS led to a 58% increase in self-care and effective coping strategies, compared to only 26% for women working on PMS alone. The same study showed 84% of women reported increased partner awareness and understanding after structured support interventions.
The key insight: your involvement is not just emotional support - it's a measurable factor in how well she manages the symptoms. When you reduce her mental load proactively, her body doesn't have to burn cognitive resources managing logistics while also managing a hormone crash. That reduction in stress compounds positively across the cycle.
The most common failure mode is inconsistency. Men who provide excellent support one month and forget entirely the next create unpredictability, which increases her stress load. The solution is tracking her cycle - not to "predict her mood" like some algorithmic weather app, but to create a consistent support cadence she can rely on.
If you're not tracking her cycle yet, start with a basic period tracker app designed for partners that sends you reminders when the luteal phase begins. The goal isn't surveillance. It's preparation.
What to Say (and What Never to Say) During PMS
The fastest way to escalate conflict during the luteal phase is to treat her emotional response as irrational or something that needs to be "fixed." She's not broken. Her serotonin is temporarily depleted, which means her emotional regulation capacity is running at 70% instead of 100%. The communication strategy that works is validation, not correction.
What Never to Say:
- "Are you on your period?" or "Is it that time of the month?" - This dismisses her experience as purely hormonal rather than acknowledging both the biological shift and whatever legitimate issue she's raising.
- "You're being crazy/irrational/too emotional" - Clinical terminology: you're telling her that her neurochemical state invalidates her perspective. That's a trust-breaking move.
- "Calm down" - Has never once in human history calmed anyone down. It signals that you view her emotional state as a problem to suppress rather than a signal to address.
- "It's not that big of a deal" - You don't get to decide the emotional weight of an issue for someone else, especially when their neurotransmitter balance is chemically altered.
- "You're overreacting" - See above. Same problem, different phrasing.
What to Say Instead:
- "That sounds really frustrating. What do you need right now?" - Opens the door for her to tell you whether she needs problem-solving, validation, or space.
- "I hear you. That makes sense." - Validation without agreement. You're acknowledging her perspective is legitimate from her vantage point.
- "I'm sorry you're dealing with this. How can I help?" - Shifts from defensiveness to partnership.
- "Do you want to talk this through, or would you rather I just listen?" - Gives her agency over the type of support she receives.
- "I'm here. You don't have to handle this alone." - Reduces isolation, which is one of the primary emotional drivers during the luteal phase.
The principle underneath all of these is simple: validation precedes problem-solving. Most men are conditioned to respond to emotional distress with solutions. During PMS, that instinct backfires because the primary need isn't a solution - it's feeling heard and not alone in the experience.
 Small changes in phrasing can dramatically reduce friction. Moving from a 'fix-it' mindset to a 'validation' mindset is the key to relational optimization during the cycle.
Small changes in phrasing can dramatically reduce friction. Moving from a 'fix-it' mindset to a 'validation' mindset is the key to relational optimization during the cycle.
Here's the tactical breakdown of how to execute this in real time:
Step 1: Pause before responding. If she says something that sounds unfair or disproportionate, your first instinct will be defensiveness. Catch that reflex. Take three seconds. Remind yourself that her baseline emotional regulation is chemically compromised right now, which doesn't mean she's wrong - it means the intensity of her response is amplified.
Step 2: Reflect what you're hearing. "It sounds like you're saying [restate her concern in your own words]. Is that right?" This does two things: it confirms you're actually listening, and it gives her a chance to clarify if you misunderstood.
Step 3: Validate the feeling, even if you don't agree with the conclusion. "I can see why that would feel overwhelming." You're not agreeing that the situation is objectively overwhelming - you're acknowledging that from her current neurochemical state, it feels that way. That's accurate, and it's enough.
Step 4: Ask what she needs. "What would help right now?" Let her direct the next move. Sometimes it's problem-solving. Sometimes it's just sitting with her. Sometimes it's giving her space.
The failure mode most men hit is skipping steps 2 and 3 and jumping straight to step 4. That reads as dismissive, even if your intent is helpful. The sequence matters.
One advanced note: if you're in a situation where you genuinely can't provide what she's asking for (she wants you to cancel work and stay home, for example), acknowledge the request and explain the constraint without defensiveness. "I hear that you need me here, and I want to be. I have a meeting I can't move, but I'll be home by 3 and I'm clearing the rest of the afternoon. Does that work?" You're validating her need while also setting a realistic boundary.
The goal isn't to become a verbal gymnast who never says the wrong thing. The goal is to shift your default response from "fix" mode to "support" mode during the 10-day window when her neurochemistry makes that support biochemically significant.
For more on how to navigate mood swings during her period, the same communication principles apply - but the hormonal drivers shift slightly once bleeding starts.
Physical Relief: What Actually Works
The most effective PMS symptom management is physical, not verbal. Pain, bloating, fatigue, and cramps are the result of prostaglandin release (the chemical that triggers uterine contractions) and fluid retention. Your role is to reduce those physical symptoms so she's not also fighting discomfort while managing the emotional component.
Heat Therapy
Heat is the single most effective non-pharmaceutical intervention for menstrual cramps. It works by relaxing uterine muscle contractions and increasing blood flow to the pelvic region. A 2012 study published in Evidence-Based Nursing found that heat therapy was as effective as ibuprofen for pain relief in dysmenorrhea (painful periods).
What to do:
- Keep a rechargeable heating pad on hand. Cordless versions let her move around instead of being tethered to an outlet.
- If she's at work or out, microwaveable heat wraps (the kind you activate by opening the package) are portable alternatives.
- Hot baths or showers provide whole-body relief and also help with the muscle tension that often accompanies cramps.
Pain Relief Medication
Over-the-counter NSAIDs (nonsteroidal anti-inflammatory drugs) like ibuprofen or naproxen are more effective than acetaminophen for menstrual pain because they block prostaglandin production. The key is timing - taking the medication at the first sign of cramps is significantly more effective than waiting until the pain is severe.
What to do:
- Stock ibuprofen (Advil, Motrin) or naproxen (Aleve) before the luteal phase starts so she doesn't have to go get it while symptomatic.
- If she's prone to severe cramps, suggest she take the first dose at the very first twinge of discomfort rather than waiting to see if it gets worse.
- Make sure she's taking it with food to avoid stomach irritation.
Hydration and Electrolyte Balance
Bloating and water retention are driven by hormonal shifts that affect fluid balance. Counterintuitively, drinking more water reduces bloating because it signals the body to stop retaining fluid. Magnesium and potassium also help regulate fluid balance and reduce cramping.
What to do:
- Keep her water bottle filled and visible. Passive hydration reminders work better than verbal ones.
- Stock magnesium-rich foods: dark leafy greens, nuts, seeds, bananas.
- Avoid suggesting diuretics (caffeine, alcohol) unless she brings them up - they can worsen dehydration and make cramps worse.
Rest and Low-Demand Environment
Fatigue during PMS isn't laziness - it's a biological response to the energy cost of managing inflammation and hormonal shifts. Sleep quality also tends to drop during the luteal phase due to elevated progesterone (which initially causes drowsiness but then disrupts REM sleep when it drops).
What to do:
- Handle tasks that would normally require her input so she can rest without guilt.
- Lower household noise and light levels in the evening to support better sleep.
- Don't schedule high-energy activities or social obligations during the 10-day window unless she explicitly wants them.
What Doesn't Work (and Why It Backfires)
- "Just push through it" - Pain and fatigue are signals of inflammation. Ignoring them doesn't make them go away; it increases stress load and worsens symptoms.
- Suggesting exercise as a cure-all - Moderate exercise can help some women by releasing endorphins, but high-intensity workouts during peak symptoms often backfire by increasing cortisol and inflammation. If she wants to move, great. If she doesn't, respect that.
- Minimizing the pain - "It can't be that bad" or "Other women handle this fine" is not just dismissive; it's factually wrong. Pain tolerance and symptom severity vary widely. Some women have cramps that meet the clinical threshold for acute pain. Believe her.
The physical relief strategy is straightforward: reduce inflammation, manage pain, support rest, and remove logistical friction. These interventions are measurable and evidence-based. They work because they address the underlying biological mechanisms rather than trying to willpower through them.
For a deeper breakdown of how to provide comfort during the entire cycle, see our guide on how to comfort your girlfriend during PMS.
Nutritional Support: Foods That Help vs Harm
Nutrition during the luteal phase isn't about diet culture or restriction - it's about stabilizing blood sugar and reducing inflammation to minimize PMS symptoms. Certain foods demonstrably worsen symptoms by spiking insulin, increasing inflammation, or depleting magnesium. Others provide the micronutrients her body is burning through faster than usual.
Foods That Help
Complex Carbohydrates Whole grains, sweet potatoes, oats, and quinoa stabilize blood sugar and support serotonin production. The luteal phase is marked by increased insulin resistance, which means her body processes glucose less efficiently. Complex carbs provide steady energy without the crash that comes from refined sugars.
Magnesium-Rich Foods Magnesium reduces cramping, supports muscle relaxation, and regulates neurotransmitter function. Dark leafy greens (spinach, kale), nuts (almonds, cashews), seeds (pumpkin, sunflower), and legumes are all high in magnesium. A 2010 study in the Journal of Women's Health found that magnesium supplementation reduced PMS symptoms in 95% of participants.
Omega-3 Fatty Acids Found in fatty fish (salmon, sardines, mackerel), walnuts, and flaxseeds, omega-3s are anti-inflammatory and have been shown to reduce menstrual pain. A 2012 study in the Journal of Psychosomatic Obstetrics & Gynecology found that omega-3 supplementation reduced both physical and psychological PMS symptoms.
Calcium and Vitamin D Calcium supports muscle function and neurotransmitter release. Vitamin D regulates mood and immune function. Dairy, fortified plant milks, leafy greens, and fatty fish are good sources. A 2009 study in Archives of Internal Medicine found that calcium and vitamin D together reduced PMS symptoms by up to 40%.
Protein Lean protein (chicken, turkey, tofu, legumes) stabilizes blood sugar and supports neurotransmitter production. Tryptophan (found in turkey, eggs, and cheese) is a precursor to serotonin, which is exactly what her brain is running low on during the luteal phase.
Foods That Harm
Refined Sugar and Simple Carbs Candy, pastries, white bread, and sugary drinks cause blood sugar spikes followed by crashes, which worsen mood swings, fatigue, and irritability. The cravings for these foods are real - serotonin depletion drives sugar cravings because sugar temporarily boosts serotonin. But the crash that follows makes symptoms worse, not better.
Caffeine Coffee and energy drinks increase cortisol (stress hormone), worsen anxiety, and can exacerbate breast tenderness and bloating. If she's a regular coffee drinker, don't suggest she quit cold turkey during PMS - caffeine withdrawal on top of hormone withdrawal is a bad combination. But reducing intake by half can help.
Alcohol Alcohol disrupts sleep, depletes B vitamins (which are already low during the luteal phase), and worsens mood swings by interfering with neurotransmitter regulation. It also increases bloating and inflammation.
High-Sodium Foods Processed foods, fast food, and salty snacks worsen water retention and bloating. The body is already holding onto more fluid during the luteal phase - adding excess sodium amplifies that.
Trans Fats and Highly Processed Foods Fried foods, packaged snacks, and processed meats increase inflammation and have been linked to increased PMS severity in multiple studies.
Practical Application
You're not her nutritionist, and suggesting dietary changes during PMS will likely backfire. Instead, the tactical move is to stock the house with helpful foods and handle meal prep so she's not defaulting to the easiest (often least helpful) option when she's symptomatic.
What this looks like:
- Prep easy, nutrient-dense meals she can grab without effort: grain bowls with roasted vegetables and salmon, overnight oats with nuts and berries, hummus and veggie sticks.
- Keep magnesium-rich snacks visible and accessible: trail mix, dark chocolate (which is also magnesium-rich and satisfies sugar cravings in moderation), bananas.
- Hydrate her passively by keeping a full water bottle within reach and refilling it without being asked.
- If she's craving sugar or salt, acknowledge the craving without judgment and offer a compromise that won't spike her symptoms as much: dark chocolate instead of candy, popcorn instead of chips, fruit instead of pastries.
The goal isn't to police her food choices. It's to reduce the friction between what her body needs and what's easiest to access when she's fatigued and symptomatic.
For more on how nutrition intersects with cycle phases, see our guide on eating for your cycle.
The Communication Pivot: Validation Over Solutions
The number one relationship fracture point during PMS is the mismatch between what she needs (validation) and what most men provide (solutions). This isn't a personality conflict - it's a neurological one. When serotonin is depleted, the brain's threat-detection system becomes hyperactive. Small issues feel bigger. Neutral statements sound critical. The baseline interpretation of ambiguous social cues skews negative.
Your job is not to fix the problem she's describing. Your job is to reduce her nervous system activation by signaling that she's not alone in the experience.
Here's the distinction:
Fix-It Mode (High Friction): Her: "I feel like I'm doing everything around here and you're just coasting." You: "That's not true. I did the dishes yesterday and took out the trash. You're not being fair."
What you've done: invalidated her perception, triggered defensiveness, escalated the conflict.
Validation Mode (Low Friction): Her: "I feel like I'm doing everything around here and you're just coasting." You: "That sounds exhausting. You're carrying a lot right now. What would help?"
What you've done: acknowledged her experience, reduced isolation, invited collaboration instead of defensiveness.
The second response doesn't require you to agree that you're "coasting." It requires you to acknowledge that from her current vantage point, it feels that way - and that feeling is biochemically amplified right now. Once her nervous system calms, you can revisit whether the distribution of household labor needs adjustment. But mid-luteal-phase is not the time for that negotiation.
The Say This, Not That Framework
| Situation | Say This (Validation) | Not That (Dismissal) |
|---|---|---|
| She's overwhelmed by small tasks | "I can see this feels like a lot right now. Let me handle [specific task]." | "It's not that complicated. Just do it tomorrow." |
| She's upset about something you don't think is a big deal | "I hear you. That's frustrating. What do you need from me?" | "You're overreacting. It's not worth getting upset about." |
| She's withdrawn or quiet | "You seem like you need some space. I'm here if you want to talk, or I can give you room." | "Why are you being like this? What did I do?" |
| She's irritable or snapping | "I can tell you're having a rough day. Do you need anything, or should I just stay out of your way for a bit?" | "You're being mean for no reason. Calm down." |
| She's crying or emotionally flooded | "I'm right here. You don't have to explain. I'm not going anywhere." | "What's wrong? Why are you crying? Talk to me." |
The underlying principle: validation reduces nervous system activation. Solutions increase cognitive load. During the luteal phase, her brain is already running at higher baseline stress. Adding more cognitive load (even well-intentioned problem-solving) makes things worse, not better.
This doesn't mean you can never address legitimate issues. It means you time the conversation for after the 10-day window when her neurotransmitter balance is restored and the conversation can happen without the emotional amplification of PMS.
The Advanced Move: Pre-Emptive Validation
The most effective partners don't wait for conflict to deploy validation - they validate proactively during the luteal phase by acknowledging the difficulty of the experience before she has to ask for it.
Examples:
- "I know this week is hard for you. I've got dinner and cleanup tonight. You don't have to do anything."
- "You've been handling a lot this month. I want you to know I see that."
- "If you need to check out this weekend and just rest, I'll handle [the thing that normally requires her involvement]."
Pre-emptive validation does two things: it signals that you're paying attention to her cycle (which builds trust), and it removes the emotional labor of having to ask for support when she's least equipped to articulate what she needs.
For more on how to navigate this communication shift across the entire cycle, see our guide on how to talk to your girlfriend during the follicular phase, where the communication strategy inverts - that's the green-light window for big conversations and problem-solving.
Long-Distance Support: How to Help From Afar
Most PMS support guides assume physical proximity. If you're long-distance, you can't bring her a heating pad or handle household logistics. But you can still provide meaningful support by reducing her emotional isolation and managing the logistics you can control remotely.
Remote Comfort Delivery
Food and Essentials:
- Use delivery apps (DoorDash, Uber Eats, Instacart) to send her comfort food without requiring her to cook or go out. Ask her ahead of time what she wants during the luteal phase, or default to her known comfort foods.
- Send a care package before the 10-day window starts: heating pad, magnesium supplements, her favorite snacks, a handwritten note. The timing matters - if it arrives after symptoms peak, it's reactive. If it arrives before, it's proactive.
- Schedule recurring grocery or meal deliveries during the luteal phase so she doesn't have to think about food procurement while symptomatic.
Emotional Presence Without Physical Presence
Check-Ins:
- Text her at predictable times during the day - not to demand a response, but to signal that you're thinking about her. "Hope you're feeling okay today. No need to respond, just wanted you to know I'm here."
- Avoid open-ended "How are you?" texts, which require cognitive effort to answer. Use specific, low-effort prompts: "On a scale of 1-5, how's your pain today?" or "Need anything delivered tonight?"
Low-Demand Connection:
- Suggest low-effort virtual activities that don't require her to "perform" - watching a show simultaneously while on FaceTime, sending her playlists or podcasts, playing a co-op game that doesn't require voice chat.
- Don't push for deep emotional conversations during peak symptoms unless she initiates. The luteal phase is not the time for relationship check-ins or difficult topics.
What Not to Do Long-Distance
Avoid:
- Making her feel guilty for not being as communicative during the luteal phase. "You've been distant this week" reads as criticism when she's symptomatic.
- Scheduling high-stakes conversations or relationship talks during the 10-day window. If something needs to be discussed, wait until after her period ends.
- Asking her to manage logistics on your behalf. If you need her to book something, coordinate something, or make a decision, either handle it yourself or postpone it.
The core principle of long-distance PMS support is the same as in-person: reduce her load, validate her experience, and create space for her to rest without guilt. The tactics shift, but the strategy doesn't.
For more on maintaining connection during challenging windows, see our guide on how to keep long distance relationship alive.
When PMS Becomes a Medical Issue
Standard PMS is manageable with behavioral interventions. PMDD is not. If your partner's symptoms meet any of the following criteria for two or more consecutive cycles, the next step is medical evaluation - not more heating pads.
Red Flags That Indicate PMDD or Other Medical Issues:
- Severe depression or suicidal thoughts during the luteal phase that resolve after menstruation starts.
- Inability to function - missing work, canceling social commitments, unable to complete basic tasks for multiple days.
- Rage or uncontrollable anger that is disproportionate to triggers and only occurs during the luteal phase.
- Panic attacks or severe anxiety that spike premenstrually and drop off after bleeding begins.
- Physical symptoms that don't respond to standard interventions - debilitating pain that ibuprofen doesn't touch, vomiting, fainting, or other acute symptoms.
PMDD is not a failure of willpower or emotional regulation. It's a neurobiological disorder that requires medical treatment, typically SSRIs (selective serotonin reuptake inhibitors), hormonal birth control to suppress ovulation, or in severe cases, GnRH agonists to induce temporary menopause.
How to Bring This Up Without Sounding Like You're Pathologizing Her
The conversation needs to frame medical evaluation as a tool for improving quality of life, not as a judgment that something is wrong with her.
What to say: "I've noticed that the week before your period is really hard for you, and it seems like it's getting worse. I read that there are medical treatments that can help with severe PMS symptoms. Would you be open to talking to a doctor about it? I want you to feel better, and I don't want you to have to white-knuckle through this every month if there's something that could help."
What not to say: "You need to see a doctor because you're impossible to be around during PMS." "I think you have PMDD. You should get that checked out." "This isn't normal. Something's wrong with you."
The goal is to position medical evaluation as a support option, not a mandate or criticism. If she's resistant, don't push. Instead, provide her with resources (links to PMDD research, a list of gynecologists who specialize in hormone disorders) and let her decide when she's ready to pursue it.
What Medical Evaluation Looks Like
A doctor diagnosing PMDD will typically:
- Ask her to track symptoms for 2-3 cycles using a daily symptom diary.
- Rule out other conditions (thyroid disorders, anxiety disorders, depression unrelated to the cycle).
- Confirm that symptoms are confined to the luteal phase and resolve within a few days of menstruation starting.
If PMDD is confirmed, treatment options include:
- SSRIs (fluoxetine, sertraline) taken either daily or only during the luteal phase.
- Hormonal birth control to suppress ovulation and eliminate the progesterone drop.
- Lifestyle interventions as adjunct support (exercise, diet, cognitive behavioral therapy).
- GnRH agonists (Lupron) in severe cases to induce temporary menopause.
Your role in this process is support, not diagnosis. You can encourage her to seek evaluation, provide logistical help (finding a doctor, going with her to appointments if she wants), and validate that seeking treatment is not a weakness - it's the same as treating any other medical condition.
For more on how to recognize when support shifts from behavioral to medical, see our guide on signs your girlfriend needs space - sometimes withdrawal during the luteal phase is biological, and sometimes it's relational, and the distinction matters.
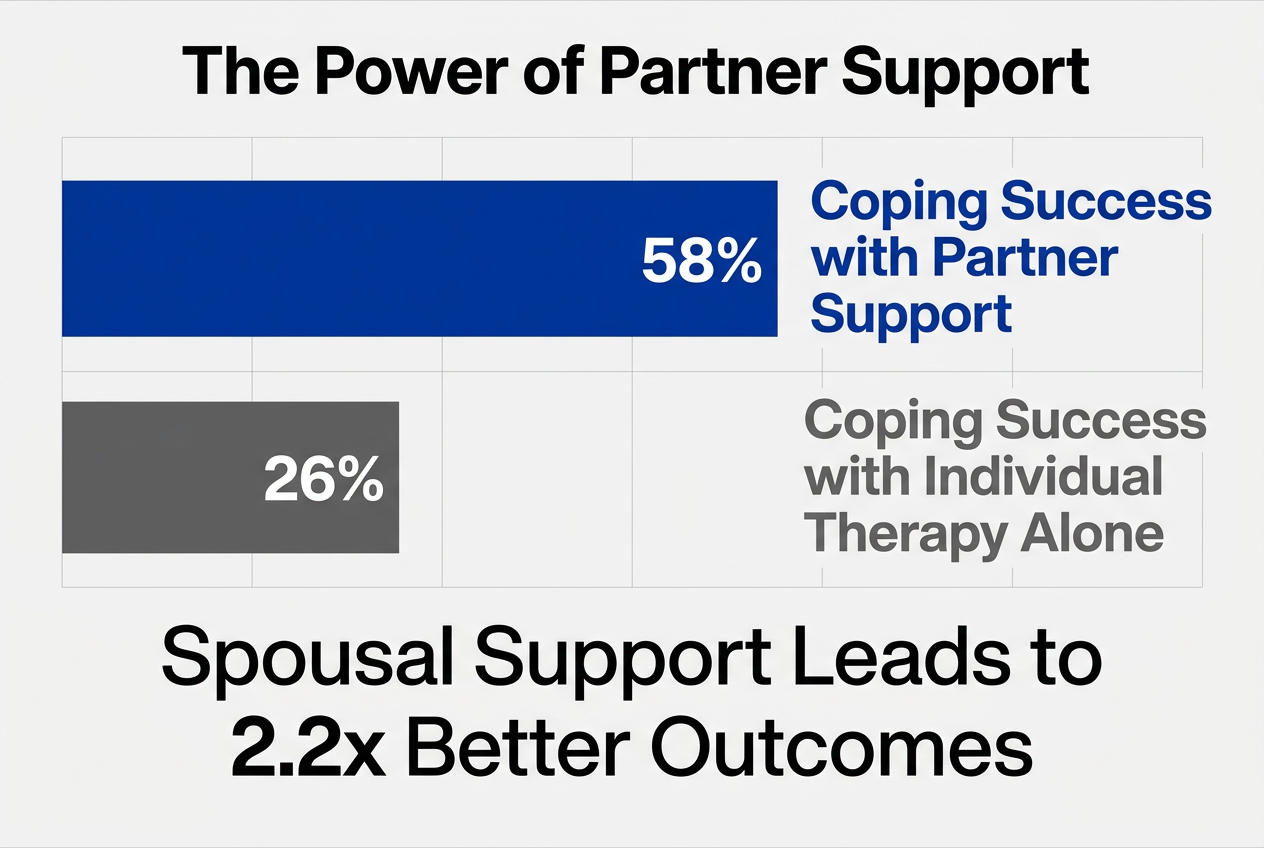 Research proves that active partner involvement is twice as effective as individual therapy in helping women manage the emotional and physical symptoms of PMS.
Research proves that active partner involvement is twice as effective as individual therapy in helping women manage the emotional and physical symptoms of PMS.
Join thousands of men using VibeCheck to track her cycle and show up better every day.
Get VibeCheck FreeFrequently Asked Questions
How to handle gf during PMS?
Handle your girlfriend during PMS by focusing on proactive support, not reactive damage control. The most effective strategy is reducing her mental load 5 days before bleeding starts - handle logistics she'd normally manage, stock comfort items ahead of time, and lower social demands. During active symptoms, prioritize validation over solutions: acknowledge what she's experiencing without dismissing it or trying to fix it unless she explicitly asks. Research from a 2017 PLoS ONE study shows that couples-based PMS interventions increased effective coping by 58% compared to individual approaches, meaning your active involvement is biochemically significant. The tactical moves: use heat therapy for cramps, keep her hydrated, handle meals without asking, and deploy the communication pivot from "fix-it" to "I'm here" mode. Consistency across cycles builds trust and reduces her stress response over time.
What is the 7 2 1 rule for menstruation?
The 7-2-1 rule is a viral social media trend that claims women experience 7 days of PMS symptoms, 2 days of peak irritability, and 1 day of complete breakdown before menstruation starts. It's biologically inaccurate. PMS symptoms typically begin 3-5 days before bleeding, not 7, and the "peak irritability" window varies widely depending on individual hormone sensitivity and serotonin depletion patterns. The rule oversimplifies a complex neurochemical process and frames women's symptoms as a countdown to inevitable irrationality, which is both dismissive and wrong. The actual science: progesterone withdrawal in the late luteal phase triggers a drop in GABA and serotonin, which affects mood regulation - but symptom severity, duration, and specific manifestations differ significantly between individuals. Some women have minimal symptoms. Others meet the threshold for PMDD, which is a clinical disorder. The better framework is the 10-day support window (5 days luteal phase + 2-7 days menstruation) and proactive strategies based on what your specific partner experiences, not a meme-based formula.
Does PMS affect relationships?
Yes, PMS measurably affects relationships - but the impact depends entirely on how partners respond to it. Research published in The Conversation (2017) found that 40% of women report moderate to severe premenstrual stress in the 3-4 days before bleeding, and that stress directly affects communication patterns, conflict frequency, and emotional availability. The key finding: when male partners are educated about PMS and provide structured support, relationship distress decreases significantly. In the same study, 84% of women reported increased partner understanding after intervention, and couples-based therapy for PMS led to a 58% increase in coping strategies compared to 26% for individual therapy. The takeaway is that PMS creates friction when it's treated as an unpredictable personality shift instead of a predictable biological event. Relationships where partners track the cycle, reduce demands during the luteal phase, and validate symptoms instead of dismissing them report significantly lower PMS-related conflict. The biological event is unavoidable, but the relational fallout is not.
Can a man help his wife during PMS?
A man can significantly help his wife during PMS, and the research shows that active male involvement is more effective than individual coping strategies alone. The 2017 PLoS ONE study found that spousal support interventions increased women's self-care and symptom management by 58%, compared to only 26% when women addressed PMS individually. The most effective strategies are logistical and emotional, not medical: reduce her mental load by handling household tasks she'd normally manage, provide physical comfort tools like heating pads and pain relievers before symptoms start, and shift communication from problem-solving to validation. The biochemical mechanism that makes male support effective is stress reduction - when a partner actively manages logistics and provides emotional validation, cortisol (stress hormone) decreases, which reduces the severity of PMS symptoms by lowering overall nervous system activation. The tactical moves: stock the house with her preferred comfort items before the luteal phase, handle meal planning and cooking during the 10-day window, give her explicit permission to rest without guilt, and validate her experience without dismissing it or suggesting she's overreacting. Consistency matters more than intensity - showing up reliably every cycle builds trust and reduces her anticipatory stress.
What can I do to help when my wife is PMS?
When your wife has PMS, the most effective help is reducing her workload and validating her experience without trying to fix it. Start by handling tasks she normally manages - meal prep, grocery shopping, coordinating schedules, household logistics - so her brain isn't burning cognitive resources on logistics while also managing a hormone crash. Physical relief comes next: provide heat therapy (heating pad, hot bath), ensure she has ibuprofen or naproxen on hand and takes it at the first sign of cramps, and keep her hydrated by refilling her water bottle without being asked. On the emotional side, validate her feelings without defensiveness: "That sounds really hard" or "I'm here, you don't have to explain" work better than "You're overreacting" or "Calm down." The data backs this up - a 2017 study found that active spousal support increased women's effective PMS coping by 58%. Avoid scheduling difficult conversations or high-demand activities during the luteal phase, and give her explicit permission to rest without guilt. The tactical playbook: proactive support before symptoms peak, validation over solutions during active symptoms, and consistency across cycles to build trust.
What should men do to help their partners during PMS?
Men should focus on three areas when helping partners during PMS: reducing mental load, providing physical relief, and validating emotions without trying to fix them. Start by tracking her cycle so you know when the luteal phase begins - approximately 5 days before bleeding - and handle logistics she'd normally manage before symptoms peak. Stock comfort items (heating pads, pain relievers, preferred snacks), cook or order meals without asking, and take over household tasks so she's not managing invisible labor while symptomatic. For physical relief, provide heat therapy for cramps (heating pad, hot bath), ensure she's taking ibuprofen at the first sign of pain, and keep her hydrated. Emotionally, shift from "fix-it" mode to "I'm here" mode: acknowledge what she's experiencing, avoid dismissive statements like "You're overreacting," and ask what she needs instead of assuming. Research from PLoS ONE (2017) found that couples-based PMS interventions increased effective coping by 58% compared to individual strategies, meaning your involvement is biochemically significant. The most common failure mode is inconsistency - showing up one month and forgetting the next. Build a predictable support cadence so she knows she can rely on you.
How to deal with PMS as a guy?
As a guy dealing with your partner's PMS, the most effective approach is understanding the biological mechanism and responding proactively instead of reactively. PMS is driven by progesterone withdrawal in the late luteal phase, which drops serotonin by up to 30% and makes emotional regulation harder. Your job is to reduce her stress load so her body isn't fighting both a hormone crash and logistical overwhelm. Start by tracking her cycle using a period tracker app with partner mode so you can anticipate the 10-day support window (5 days before bleeding + the period itself). Proactively handle tasks she'd normally manage, stock comfort items before symptoms start, and lower social and emotional demands during that window. When conflict arises, validate instead of defending: "That sounds frustrating, what do you need?" works better than "You're being unfair." Research shows that male partners who provide structured support reduce PMS-related relationship friction by 58%. The tactical moves: heat therapy for cramps, hydration without nagging, validation without problem-solving, and consistency across cycles. The goal isn't perfection - it's showing up reliably so she knows she's not managing this alone.
What are the signs that PMS has become a clinical issue requiring a doctor?
PMS becomes a clinical issue requiring medical evaluation when symptoms prevent normal functioning for two or more consecutive cycles. The red flags: severe depression or suicidal thoughts during the luteal phase that resolve after menstruation starts, inability to work or complete daily tasks, rage or panic attacks confined to the premenstrual window, or physical pain that doesn't respond to over-the-counter medication. These symptoms indicate PMDD (premenstrual dysphoric disorder), which affects 3-8% of menstruating women and requires medical treatment - typically SSRIs, hormonal birth control, or GnRH agonists in severe cases. Standard PMS affects 90% of women and responds to behavioral interventions like rest, heat therapy, and stress reduction. PMDD is a DSM-5 mood disorder and does not. If your partner is missing work, isolating from friends, or experiencing suicidal ideation premenstrually, the next step is evaluation by a gynecologist or psychiatrist who specializes in reproductive mental health, not more heating pads. Frame the conversation as support, not criticism: "I've noticed this is really hard for you every month. Would you be open to talking to a doctor about treatment options?" Do not diagnose her yourself, but do provide resources and encourage her to track symptoms for 2-3 cycles so a doctor can assess the pattern.
How to support my partner if we are long-distance?
Long-distance PMS support focuses on reducing emotional isolation and managing the logistics you can control remotely. Use food delivery apps (DoorDash, Uber Eats, Instacart) to send her comfort meals during the luteal phase so she's not managing food procurement while symptomatic. Send a care package before the 10-day window starts - heating pad, magnesium supplements, her favorite snacks, a handwritten note. Timing matters: if it arrives proactively, it signals you're paying attention; if it arrives reactively, it's damage control. On the emotional side, text her at predictable times with low-effort prompts: "On a scale of 1-5, how's your pain today?" or "Need anything delivered tonight?" instead of open-ended "How are you?" questions that require cognitive effort to answer. Avoid scheduling high-stakes relationship conversations or demanding her attention during peak symptoms. Suggest low-demand virtual connection: watching a show simultaneously on FaceTime, sending playlists, or co-op gaming that doesn't require voice chat. Do not make her feel guilty for being less communicative during the luteal phase - frame it as normal and expected. The principle is the same as in-person support: reduce her load, validate her experience, create space for rest without guilt. The tactics shift, but the strategy doesn't.
Tags

Related Articles
Continue reading to deepen your understanding

How to Know Girlfriend Luteal Phase Mood Changes (2026)
Understand how to know girlfriend luteal phase mood changes using the 5-7 day early warning window and 28-day cycle tracking to reduce relationship stress.

How to Predict Girlfriend Mood Swings by Cycle (2026)
Learning how to predict girlfriend mood swings by cycle reduces relationship friction by 58% using this tactical four-phase hormonal support system now.

How to Help Your Girlfriend During Ovulation Week: A Partner’s Playbook
Has she suddenly hit peak energy? That’s her biological summer. Learn how to navigate her cycle and support her social and creative spikes during ovulation week.

The Proactive Partner’s Guide to the Menstrual Cycle Phases
Stop walking on eggshells and start understanding the 28-day loop. This guide helps you anticipate her needs and become the partner who shows up exactly when she needs you most.

How to Tell Which Cycle Phase Your Girlfriend Is In: A Guide for Partners
Stop guessing why her mood shifted. Learn to recognize the behavioral patterns of her menstrual cycle so you can be a more supportive partner and reduce relationship conflict by 58%.

The Luteal Phase Playbook: A Man’s Tactical Guide to Supporting His Partner
Is she crying about milk or questioning your entire future? It might be the luteal phase. Learn the biology behind the mood shifts and how to be the partner she actually needs right now.
App ciclo menstrual para parejas: Best Trackers (2026)
Find the best app ciclo menstrual para parejas to boost your bond. We ranked top tools by tactical missions for men and data privacy for 2026 results.
Boyfriend Guide to Menstrual Cycle Phases & Support
Learn how to navigate the four menstrual cycle phases with this essential guide for men. Improve communication, reduce friction, and provide proactive support.